

Rural Health Workforce Transformation Needs More Than Bonuses
At Nurse Recruitment Experts, we spend our time inside the challenges of rural hiring, helping small hospitals attract clinicians, helping families relocate, and helping states understand what it really takes to build a workforce that stays. Across all of this work, one truth keeps emerging.
You cannot bonus your way out of a rural workforce crisis.
You have to build your way out.
This month Iowa underscored just how urgent the situation has become. The state’s Department of Health and Human Services released a notice of intent for an RFP focused entirely on workforce. In Iowa’s 2025 statewide survey, hospitals identified clinical recruitment and retention as the number one need for investment.
The state is preparing to use one-time incentives, relocation support, and a five-year service requirement to stabilize rural communities. And Iowa is not the only one. Across the eighteen RHTP applications we reviewed, including Alaska, Oregon, Idaho, Arizona, Montana, Nevada, Texas, North Dakota, New Mexico, Wyoming, Washington, California, Colorado, Kansas, and Utah, one theme stands out.
- Rhetoric on recruitment incentives, like relocation bonuses.
- Rhetoric on 5-year commitments.
- Light investment in long term retention systems.
States are preparing to move clinicians. Without a different strategy, they will struggle to keep them. This is why Rural Health Workforce Transformation Needs More Than Bonuses is not just a message but a warning.
The Bonus Problem
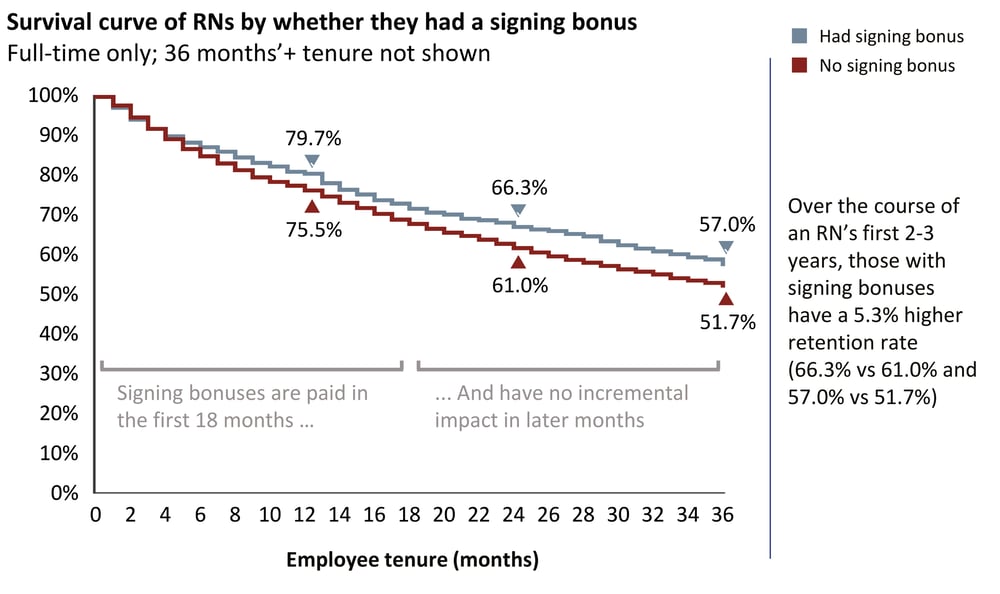
National data from Laudio offers one of the clearest views into what money can and cannot do.
Laudio found that:
-
Signing bonuses increase two year RN retention by only 5.3 percent
-
That improvement is worth about $2,800
-
Yet many rural hospitals now offer $15,000 to $20,000
The return on investment simply does not hold.
A bonus can help someone say yes.
A bonus can help someone afford to move.
A bonus can help a candidate choose one offer over another.
But a bonus cannot:
-
fix burnout
-
stabilize chronically short-staffed teams
-
create available housing
-
help spouses find work
-
solve childcare shortages
-
build belonging or connection
-
strengthen culture
-
reduce professional isolation
-
help someone feel at home in a rural community
In other words:
Bonuses are a tactic.
Rural workforce stability is a system.
States continue to invest in the tactic and hope it will produce a system level result. This is another reason Rural Health Workforce Transformation Needs More Than Bonuses is more than a slogan. It is a shift in thinking.

Why Relocation Incentives Alone Are Not Enough
Relocation incentives do something valuable. They reduce friction. They offset the cost of uprooting a family. They help rural employers compete with urban systems.
But nearly every RHTP application reveals the same gap.
Relocation incentives do not address the non financial reasons people leave.
A clinician will not stay for five years if their partner cannot find work or if childcare is unavailable or if housing is scarce or if onboarding is inconsistent or if burnout is overwhelming or if they feel socially isolated in a small town.
Relocation is not a transaction.
It is a transition.
Right now most states are paying for the transaction and skipping the transition.
Five Year Service Terms Only Work If You Sell the Community
Iowa is preparing to require a five year service commitment. Other states are considering similar terms.
But you cannot pay someone enough to commit five years of their life to a place they do not feel connected to.
People stay because they feel welcomed, known, supported, and integrated. They stay when the community feels like a place where their family can thrive. They stay when they can visualize a life beyond the hospital parking lot.
States like Montana, Oregon, North Dakota, and Kansas all acknowledge these issues in their RHTP applications. They reference community integration, rural quality of life, housing limitations, limited school capacity, partner employment barriers, professional isolation, and the emotional strain on rural staff.
These issues are not solved by bonuses. They are solved by systems, storytelling, and belonging. This is why Rural Health Workforce Transformation Needs More Than Bonuses must guide how states design their programs.
The Real Strategy: Sell the Town Not the Transaction
Clinicians do not stay simply because they are paid to. They stay because they build a life.
The rural employers with the strongest retention rates all do the same things. They focus on belonging.
They provide community tours for families. They offer personalized onboarding. They help clinicians find housing, schools, churches, and social groups. They introduce them to local networks. They support spouses with job connections. They offer cultural immersion that helps people understand the rhythm of rural life. They communicate transparently. They build realistic workloads that do not burn people out.
These efforts are not expensive.
They are intentional.
And they turn five year obligations into five year opportunities.
What This Means for RHTP States
RHTP is a historic moment. States have an opportunity to build the foundations of rural workforce stability. But if they invest only in incentives, they will repeat the same cycle rural health has experienced for decades.
States must invest in:
-
community onboarding
-
digital storytelling and lifestyle marketing
-
rural lifestyle branding across regions
-
childcare and housing navigation
-
spousal employment support
-
rural leadership development
-
burnout mitigation and team redesign
-
structured retention systems
This is how Rural Health Workforce Transformation actually happens. By building systems around people rather than payments.
The Opportunity Ahead
The early RHTP applications show that states are ready to invest. What they need now is a shift in strategy.
Money matters.
But money is not enough.
Rural Health Workforce Transformation Needs More Than Bonuses because rural America needs more than transactions. It needs better storytelling. It needs better community integration. It needs the systems that make staying feel natural, not contractual.
When states invest in the things that help clinicians feel at home, five year service terms stop looking like obligations. They start looking like opportunities to build the kind of life only rural communities can offer.

Founder of the Rural Healthcare Transformation Hub @ Nurse Recruitment X
Looking to secure Rural Health Transformation Program funds and fix your workforce shortages? Our Rural Health Transformation Hub helps rural hospitals, clinics, and home care agencies design winning proposals and build the pipelines needed to recruit and retain staff. We combine grant support with real recruitment expertise, giving you a low-risk way to compete for funds and implement workforce solutions that work.







